Heart Tests: Coronary angiogram - Invasive
Here's part twenty of our series entitled the heart of the matter. Part 19 is here and the disclaimer is here.
This was accidentally discovered by Sones in 1965 at the Cleveland clinic angiogram laboratory, when he accidentally injected dye into the right coronary artery, got some nice pictures, and the patient survived. You must understand that before 1965, it was considered anathema to instrumentate the coronary artery as it was thought to be fatal. The heart was sacred.
With Sones showing us the way in 1965, we have now developed a whole new field of cardiology called interventional cardiology. We boldly intervene inside the coronary arteries, saving many lives (more about that later).
Heart arteries are very small, 2-3 mm in diameter, and so the common X-rays cannot see it. Therefore to visualize the heart arteries, we need to pass a small rubber tube (catheter) into any of the major arteries eg femoral artery or radial artery, of the body (they all lead to the heart ultimately), and with the X-ray screening to guide us, move the rubber tubing (catheter) carefully into the opening of each of the major heart artery, magnify the artery, inject dye (contrast material) to outline the artery, and take pictures. As the arteries twist and turn unpredictably, it is often necessary to change our angles to try and film the artery in the right profile. Although there are standard views to take, we need to individualise for the patient.
We learn that no two persons artery flow exactly the same course. Some are longer, some shorter, some turn acutely, some turn gently, some have big branches, some smaller branches, some arise nearer the opening, some further, etc. All these variations must be adjusted for having seen the preceding shots. At the end of the picture taking, all pictures are stored in a CD (previously 35mm cine-films). The coronary angiogram usually takes a half hour, in experienced hands. The information obtained is invaluable.
The coronary angiogram is invasive, as it requires us to puncture an artery, and so requires the subject to be hospitalized for 6 hrs at least, if not overnight. There are potential problems with dye allergy and bleeding. There are also potential complications of heart attacks and strokes. There is a small (0.1%) risk of death.
Therefore, we do not advice coronary angiogram simply but only for those who have signs and symptoms of CAD or a high likelihood of CAD. We feel that if the patient has a disease (CAD), the 0.1% risk of death is worth taking, in the hope of helping him avoid a higher risk of death from CAD. With coronary angiogram, there is also the question of radiation. It is an X-ray technique. The radiation is about 500 chest X-rays. In a patient with CAD, the risk/benefit ratio is heavily in favour of the angiogram. If the patient does not have CAD (just for screening), then the risk/benefit ratio is not in favour of an angiogram.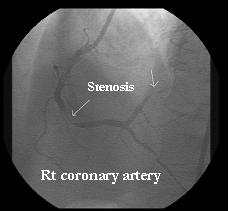 This is an example of a coronary angiogram showing stenosis in the right coronary artery.
This is an example of a coronary angiogram showing stenosis in the right coronary artery.
It must also be said that there are definite benefits from a coronary angiogram. You do make a definite diagnosis (coronary angiogram is the gold standard). It allows us to decide what is the best treatment strategy, and if angioplasty is the best strategy, it can also (if the patient and doctor wishes), be performed at the same seating. Diagnosis and management together.
Part 21 discussing non invasuve angiograms is here.
![]()
No comments:
Post a Comment