Case study on heart attack
This is a case study on heart attack and forms part thirteen of our series, the heart of the matter. Part twelve can be found here. Most of our readers should have already seen our disclaimer here.
Mr C is a 40 year old Chinese salesman, who works very hard and is under much stress to sell. He suffers from mild hypertension and is under treatment, though not very regular. One month ago, while jogging, he experience an unusual, tight band-like discomfort, over his chest. He began to sweat profusely, cold sweat. He felt dizzy. Realizing that something was not right, he called his colleague who was nearby, to come and help him. While he rested in the car, the colleague informed Mr C's wife, and drove him to the emergency room of a nearby medical center.
An ECG done there confirmed that he had indeed taken a heart attack. Mr C's ECG on arrival at emergency room, showing acute ST elevation suggestive of acute myocardial ischemia.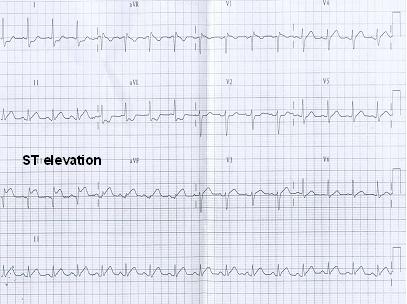
The cardiologist there decided to perform an immediate angioplasty (primary angioplasty). Mr C had total occlusion of his LAD artery. This was treated with a coronary stent. He had chest pains at about 10am. He reached the medical center at 11.30am, and the cardiologist opened the artery and implanted the stent at about 12.30noon (2hrs 30mins after the onset of chest pains). He was discharged about three days later showing full recovery of the heart muscle that was initially damaged. His ECG was virtually normal.
In the next part of the series we will be covering various checks.
![]()
3 comments:
correct me if i am wrong, but i can see st elevations most prominent on leads II,III and aVF. isn't that an inferior MI and in this case the Right coronary artery should be obstructed? on the other hand, the st segments on the chest leads are not significantly elevated as to be consistent with a total occlusion of the LAD.Could you pl explain?
http://hmatter.blogspot.com/2006/03/further-clarification-on-case-study.html
Post a Comment