64 Slice MSCT, the Srawak Experience
We had written earlier, in February, about the 64MSCT, friend or foe. Well the Sarawak General Hospital have had 64MSCT since 2004, and the specialist there did what we were hoping all centers with a new 64MSCT will do, correlate their reading of the 64MSCT non invasive coronary angiogram with the gold standard invasive coronary angiogram, so that we know their accuracy, since it takes experience and a learning curve to get good, consistent results with the 64MSCT.
We have always said that, just because others, overseas, can read a 16MSCT with reasonable accuracy, does not mean that you (after a 2 weeks or less training overseas) can read a 64slice MSCT and begin to be an expert in 64MSCT. At least the doctors in Sarawak took the trouble to establish their experience, the Sarawak experience. Their work was recently published in the Geriatric Journal of Cardiology, March 2006, entitled "Accuracy of 64 MDCT in detecting CAD in 134 symptomatic patients: the influence of calcification". Dr KH Sim and team at SGH, studied 134 patients with symptomatic CAD with their 64MSCT and then angiogram them, to correlate their accuracy, using the coronary angiogram as the gold standard. They found that calcification was a big confusing factor, so they divided their study into one group - (group A) with a lower calcium score (calcium score <142)>142). What they found is summarised in the table.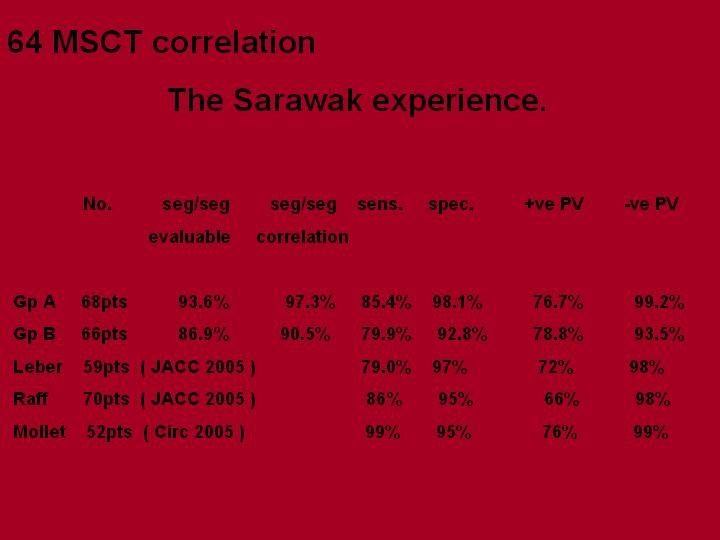
Please note that the Sarawak experience is comparable with international standards like Leber, Raff and Mollet. The sensitivity and positive predictive value is still rather variable and are low. The positive predictive value can be as low as 66% or only as high as 76%. This is surely not good enough as a costly screening diagnostic test with known radiation danger. It appears that as with universal experience, a high calcium score, heart rate >60 beats/min, and vessels < 1.5mm in diameter are still confounding and confusing factors with the 64MSCT. At the moment, it would appear that this scan machine is more harm than good, considering that one could receive a radiation dose equivalent to 500CXRs, when the positive predictive value is only 66-76%.
But not to worry, the 256slice MSCT by toshiba is on the way. The prototype is being tested in 2 Japanese and 2 American medical center.Corridor talk is that it is a much better machine for non-invasive coronary angiogram, with a lower radiation dose, being able to scan the whole heart in one heart beat with less calcium problems. So hope is on the way.
![]()
1 comment:
Have just had a clinical experience that anecdotally supports the limited correlation of CT and cath. The patient did have heavy calcification on CT and was read as having > 50 LAD, 75 RCA and 30 Cx. On cath he had total occlusion of LAD and RCA with non-obstructive dz in the Cx.
The CT was done at an outside facility, so not sure who did the interpretation; our physicians did not review the CT.
The chief of our cardiology department thinks that CT angio may be a good screening exam in patients who present with non-typical CP that is not clearly cardiac - the usual pt that would be admitted with R/O MI.
Do you see that as a possible use?
Post a Comment