What can happen in heart attacks. VIP as an example
Patients with chest pains and heart attacks are warded in CCU (coronary care unit) because of the danger of ventricular fibrillation, an event which can happen soon after a heart attack. A heart attack essentially means that there is a blocked heart artery (the background blockage is invariably due to cholesterol deposits in the heart artery), with a crack in the cholesterol deposits (plaque rupture).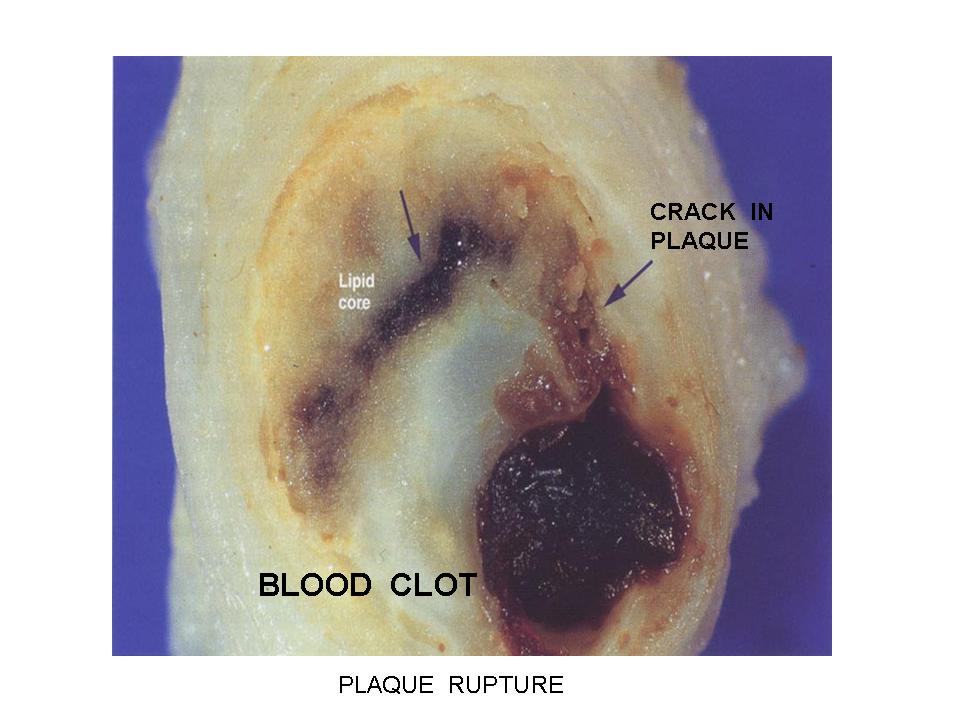 A crack in the cholesterol deposits will expose the cholesterol deposits to the flowing blood, allowing a clot to form, which blocks off the heart artery completely.With the complete blockage of the heart artery, the heart muscle that the artery supplies is deprived of vital life giving blood, and so the heart muscle dies (necrosis is our term). When heart muscle dies, it becomes very irritable and can easily fribrillate, resulting in the heart stopping (sudden cardiac death), and the patients dies, unless he is defribrillated (using a mechanical defibrillator).
A crack in the cholesterol deposits will expose the cholesterol deposits to the flowing blood, allowing a clot to form, which blocks off the heart artery completely.With the complete blockage of the heart artery, the heart muscle that the artery supplies is deprived of vital life giving blood, and so the heart muscle dies (necrosis is our term). When heart muscle dies, it becomes very irritable and can easily fribrillate, resulting in the heart stopping (sudden cardiac death), and the patients dies, unless he is defribrillated (using a mechanical defibrillator).
This is probably why Mahathir is in CCU, so that this can be detected early and defibrillation done. The risk of dying then is minimal. The other use of CCU, besides monitoring for cardiac electrical instability, is to watch out for heart failure, and manage it under constant cardiac monitor. Heart failure is another known complication of heart attacks. When heart attacks result in large amount of heart muscle damage, the heart begins to fail as a muscle pump. The damaged heart muscle is weak, and so it cannot pump hard enough to maintain the circulation.
A lesser complication of this is heart failure, meaning that the heart can pump enough to keep some circulation, but not full circulation, so that the patient experiences breathlessness, and lung congestion. We call this pulmonary congestion or edema. This can be managed with medical therapy. The prognosis is guarded as there is a mortality risk of 20-30% (Heart failure following a heart attack).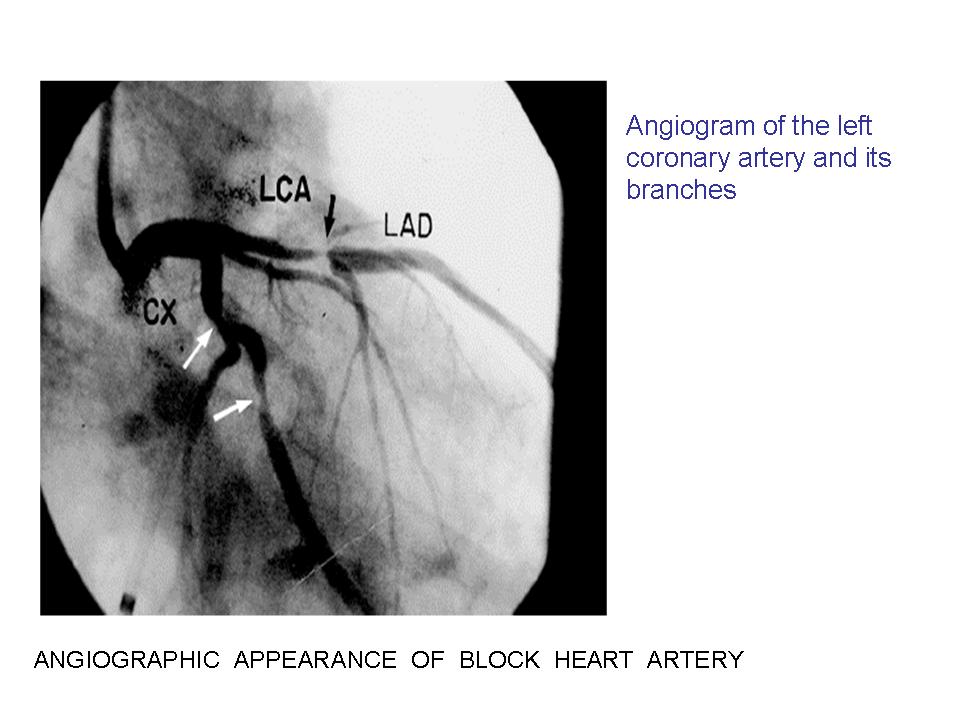 Sometimes, the heart muscle damage is so severe that the heart fails totally, and the patient goes into shock. The prognosis here is poor as the risk of dying is 80-90%, unless managed expertly with the use of emergency angioplasty or surgery, and the use of a mechanical aortic balloon pump to support the circulation. With a mild heart attack, this would seem unlikely. As long as the diagnosis is a small (mild) heart attack, the prognosis should be good even bearing in mind that he is 80years old and diabetic with previous CABG.
Sometimes, the heart muscle damage is so severe that the heart fails totally, and the patient goes into shock. The prognosis here is poor as the risk of dying is 80-90%, unless managed expertly with the use of emergency angioplasty or surgery, and the use of a mechanical aortic balloon pump to support the circulation. With a mild heart attack, this would seem unlikely. As long as the diagnosis is a small (mild) heart attack, the prognosis should be good even bearing in mind that he is 80years old and diabetic with previous CABG.
![]()
No comments:
Post a Comment