Case Study -W
Mr WCK is a 50year old Chinese male, who smokes 20 cig daily for the last 20 years, and who suffers from hypertension for the last 5 years. On the day of presentation, he experienced severe jaw tightness, with cold sweat, while walking up the stairs to his office. He rested for 15 mins in his office, and the jaw tightness slowly improved. He managed to work, but on driving home at about 7pm, the jaw tightness returned, and he perspired again. Sensing that something was not right, he decided to drop by the medical center for a check.
On P/E, the BP 130/80, HR 100/M. Precordial examination revealed a third HS. The lungs showed bilateral basal crepitations.
The ECG was done. The Troponin T was slightly positive.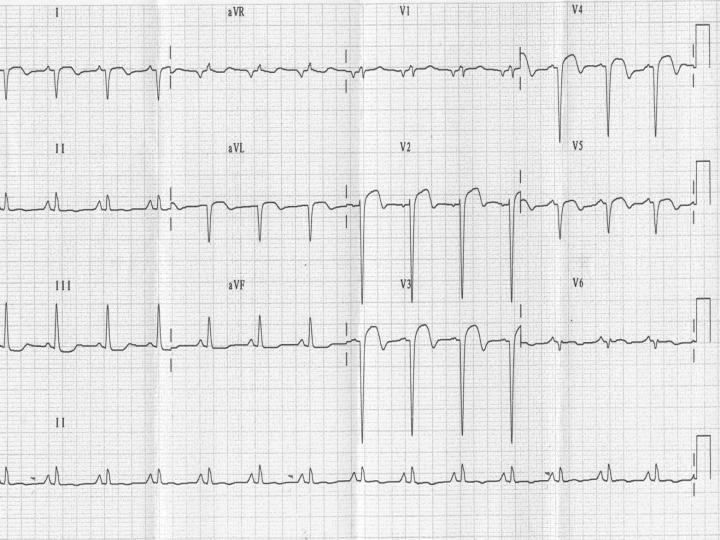
Q 1. What does the ECG show ?
Q 2. What is your diagnosis?
Q 3. How would you manage this patient?
Q 4. What is his In-hospital, and long term prognosis?
![]()
2 comments:
Q 1. What does the ECG show ?
ST segment elevation from leads V2-V5, I and AVL with Q-waves on leads V3 to V5 suggestive of an anterior septal STEMI. The rate was around 90 bpm, regular and was in sinus rhythm with upright p-waves. There was a right-axis deviation (around +135), and signs of right-atrial enlargement (tall p-waves on lead II).
Q 2. What is your diagnosis?
Heart failure secondary to an anterior septal MI that has developed more than 18 hours ago (presence of Q-waves).
Q 3. How would you manage this patient?
Immediately: sublingual nitrate if not already given; positioning sitting up; patient-administered morphine up to 10mg if in pain; aspirin 300mg; O2 high flow (8-10L/min); enoxaparin (Clexane) 1mg/kg OR consider unfractionated heparin; cardivelol; frusemide IV.
Also:remove patient shirt for later access to chest, place on constant O2 sats, ECG and BP monitor, large bore IV access, bloods for FBC including WBC diff, trop, CK/CKMB, lipid, glucose, group and save; alert/refer cardiologists. Establish resus status for patient, next-of-kin/power of guardianship/attorney.
Since the MI has probably been around for >18 hours, there is very little that can be done in terms of immediate-term thrombolysis or PCA. However, a coronary angiogram should be done, and IV abciximab/GPIIb/IIIa agents might be indicated per discussion with cardiologists in preparation of angiography +/- stents.
Consider admit for 1 week under cardio, as most MI complications would occur within that time-frame.
Consider ACEI e.g. ramipril, statins e.g. simvastatin as long as total cholesterol >2, spironolactone (aldosterone antagonists) and 100mg/day maintenance aspirin or clopidogrel if cost not an issue. If this is a recurrent MI, consider aspirin+clopidogrel combination if no previous strokes/CVAs.
Counselling on smoking cessation, dietary (reduce salt, drink in moderation) and lifestyle modifications should be done prior to discharge with follow-up with GP.
Q 4. What is his In-hospital, and long term prognosis?
Not sure. My best guess would be:
STEMI in general has a death of around 10% per episode (?), with additional chances of developing complications such as cardiogenic shock (high mortality), LV aneurysm/rupture/tamponade, pericarditis (Dressler's), chordae rupture or papillary muscle tear, and recurrent MI. MI's recur at around 10%/year with the additional chance for dying again.
Q1 correction. ST segment elevation from leads V2-V5, I and AVL with Q-waves on leads V3 to V6 suggestive of an *anterolateral* STEMI. The rate was around 90 bpm, regular and was in sinus rhythm with upright p-waves. There was a right-axis deviation (around +135), and signs of right-atrial enlargement (tall p-waves on lead II).
Post a Comment